Regardless of your thoughts about Fung … you should read this post with an open mind.
We should always question everything!! … question every thing.
I was in the midst of researching Dr. Jason Fung’s latest work for a post when Dr. RD Dikeman tagged me on this post from Jeff Cyr. Jeff’s analysis is excellent!
He does a better job than I would do, so with his permission I’m sharing it in it’s entirety. Thank YOU Jeff for sharing this information and for allowing me to share it.
Problem
by Jeff Cyr
I recently read an abstract paper about the case of a male T2D patient treated at the Intensive Dietary Management Clinic in Scarborough, Ontario, over a 4-month period. This is the Clinic run by Dr. Jason Fung. Here is the link to the paper.
✅https://journals.co.za/content/journal/10520/EJC-d7f1f32f5… .
This patient started off with a Hemoglobin A1C of 7.7%, which is an average blood glucose of 197 mg/dl if you use the correct mathematical equation to convert the A1C to average blood glucose, the DCCT formula. After 4 months of treatment, A1C was lowered to 7.2% which is an average blood glucose of 179 mg/dl. I have some serious issues with the treatment of this T2 diabetic. I will try and explain. First from the paper.
✅”This case follows a male T2D patient treated at the Intensive Dietary Management Clinic in Scarborough, Ontario, over a 4-month period. The patient’s initial fasting regimen consisted of a 24-h fast, three times a week. Over the course of treatment, the patient gradually extended his fasting period, eventually fasting for 42 h, two to three times a week. By the end of treatment, the patient’s weight was reduced by 17.8% and his waist circumference was reduced by 11.0%.
In addition, the patient’s glycated haemoglobin levels decreased from 7.7% to 7.2%, and he was able to completely discontinue his insulin treatment, despite over a decade of insulin usage. The patient did not find it difficult to adhere to the fasting schedule and did not experience any hypoglycaemic episodes or other significant adverse effects.”
With T2 diabetes we have the problem of glucolipotoxicity.
The concept of glucolipotoxicity refers to the combined, deleterious effects of elevated glucose and fatty acid levels on pancreatic beta-cell function and survival.
✅https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2824006/ .
If the picture below doesn’t make sense, don’t worry. Jeff explains it very well … in English. :)
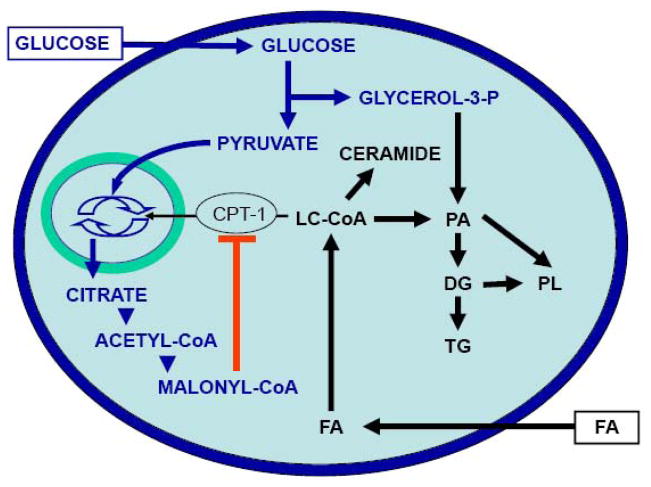
” The permissive effect of elevated glucose on the detrimental actions of fatty acids stems from the influence of glucose on intracellular fatty-acid metabolism, promoting the synthesis of cellular lipids. The combination of excessive levels of fatty acids and glucose therefore leads to decreased insulin secretion, impaired insulin gene expression, and beta-cell death by apoptosis, all of which probably have distinct underlying mechanisms.”
✅https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2824006/ .
With T2 diabetes we have the problem of severe insulin resistance directly on the fat cells in the adipose tissue. Insulin cannot properly regulate the release of fatty acids from the insulin resistant fat cells. These excess fatty acids are delivered to the liver where they contribute to liver insulin resistance, liver inflammation.
” The inhibitory effects of chronically elevated fatty acid levels has been clearly demonstrated in several studies, at least in individuals genetically predisposed to developing type 2 diabetes. It is therefore likely that glucolipotoxicity contributes to beta-cell failure in type 2 diabetes as well as to the decline in beta-cell function observed after the onset of the disease.”
✅https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2824006/ .
In my opinion they should have normalized this persons blood glucose levels first. If necessary, give insulin to normalize blood glucose and foster beta-cell recovery. You rest the beta-cells, you stop the beta-cell death from the glucolipotoxicity. The constant elevated blood glucose/fatty acid levels. You will also stop the excess production of toxic ceramides which also kills beta-cells.
Put patient on a low-carb, adequate protein, SOME healthy fats diet. Also use daily shorter intermediate fasting regime, use exercise. Resistant training, walking, biking, yoga, whatever form of exercise the patient would stick with.
In my opinion, this patient would have lowered his A1C much lower than only 7.7 to 7.2% in 4 months time. He would have also saved much more of his beta-cell mass, beta-cell function.
I realize that some folks reading this short post, may not like my public criticizing of Dr. Fung from this published paper by Dr. Fung himself.
I felt that I should bring this to folks attention. I believe that all diabetics deserve the best treatment possible.
I also believe that Dr. Richard Bernstein would agree with everything that I just stated.
Fung’s Protocols Are Harmful
I wholeheartedly agree with Jeff’s analysis. Thanks again to Jeff for writing this critique and for allowing me to share. Follow Jeff Cyr on Facebook!
It takes a lot of ‘guts’ to criticize Fung, a so-called ‘low carb expert’.
I know, I’ve written two post criticizing Fung personally and his protocols. :)
Fungus Among Us
What the Fung
I’ll close with this.
Our bodies are designed to maintain a tight range of blood sugars. Too high and insulin is secreted. Too low and our bodies produce glucose. It’s designed that way for a reason. Elevated blood sugars are toxic to every cell in the body.
Every person on the planet should obtain and maintain truly normal blood sugars. Fung disagrees. He believes elevated blood sugars are ‘fine’.
The truth is out there… but you have to find it. Let your meter be your guide.